INTRODUCTION
Smoking is a global health problem. According to the WHO report, deaths caused by smoking will rise to 8 million by 2030, which will be worse in developing countries1. Shisha smoking (SS) in the Middle East is known as a traditional way of consuming tobacco, and its consumption has increased significantly in recent years2.
Recent studies show that the prevalence of shisha smoking (SS) among Middle Eastern adolescents ranges from 6% to 34%, and among American adolescents 5–17%3. The lower age of SS and the popularity of shisha in adolescence, especially in females, have become major concerns4 as young females view SS as a hobby5. The results of the latest national survey of risk factors of non-communicable disease (SuRFNCD-2007) in Iran showed that more than half of female tobacco users are shisha consumers6. The World Health Organization (WHO) has attributed the increased tendency to shisha smoking in adolescents to misunderstandings about its harmlessness compared to other tobacco products7. In Middle East countries, people have not acquired negative attitudes toward SS, and it is much more acceptable in society than other types of tobacco. The prevalence of respiratory diseases in female smokers of shisha is higher than in male smokers8,9. Besides, complications such as changes in menstrual function, lower bone density and estrogen-deficiency disorders are the adverse effects of SS in women that require more dedicated attention10. In their study in the Eastern Mediterranean region, Afifi et al.11 showed that identifying predictors of SS among women is essential for planning future interventions to control SS among them and the community at large. It is important to understand the determinants (e.g. social norms and specific beliefs) of adolescents’ inclination to engage in this risky behavior12.
Predictors of high-risk behaviors in adolescents can be determined through the Prototype-Willingness Model (PWM). This model has the ‘reason’ and ‘social reaction’ paths. The former (reason path) shows that young people, with previous will and plan, decide to engage in risky behaviors13. Most behavioral models are based on the premise that the intention for a behavior is the result of deep thought, which needs to be scrutinized. A decision then must be made whether or not to do it14. This path includes the two variables of ‘attitude’ and ‘subjective norms’, which predict the behavioral intention as outlined in the Theory of Reasoned Action (TRA) and the Theory of Planned Behavior (TPB). According to this path, the youth who have a positive attitude towards smoking and their perceived subjective norms will predict their smoking behavior including the strong determination to start smoking and most likely initiation of use of tobacco products15.
The ‘social reaction’ pathway comprises two factors: the prototype or the mental images of people involved in the high-risk behavior, and the willingness to do it in certain situations. This path is less intentional, and the decision-making process is often unintended, with behavioral willingness playing a role in performing high-risk behaviors13.
Willingness is more easily ‘moved’ by situational influences16. A teenager is more likely to display a behavior in a facilitative situation without any prior planning or intention (for example, at a party with friends where alcoholic beverages and shisha are available). This practice is especially noticeable among young people and adolescents who are sensitive to social influences17,18.
According to PWM, behavioral willingness is associated with people’s prototype. A positive prototype toward an individual involved in the highrisk behavior reinforces the willingness to do it19. The use of the PWM model is effective in predicting high-risk behaviors such as taking illicit drugs, highrisk driving, smoking and alcohol consumption in adolescents and young adults20. Therefore, this study was conducted to determine predictors of shisha smoking among adolescent females in western Iran based on PWM.
METHODS
Study design and setting
This cross-sectional study was carried out on 1302 middle and high school females aged 12–18 years in Kermanshah, one of the largest cities with the highest prevalence of tobacco use in Iran, between January and August 2019. The method applied was multistage sampling with a systematic random approach. Initially, a list of schools in the three districts of Kermanshah was prepared. In total, 12 schools were then selected by systematic random sampling (two middle schools and two high schools). At the school level, systematic random sampling was also selected based on the number of students and the proportion of the total sample size. Written informed consent was obtained from students aged ≥16 years, and from parents of students aged <16 years. The names of the participants in the questionnaire were not recorded and other information was kept confidential and used only for this study. The Ethics Committee of Hamadan University of Medical Sciences approved this study (Ref. No.: IR.UMSHA.REC.1397.696).
Questionnaire
The data collection tool was a researcher-made questionnaire that was designed by a comprehensive review of research, literature and the results of qualitative studies (Supplementary file). The questionnaire consisted of three general sections: sociodemographic questions, questions related to SS behavior, and PWM structures. The formal and content validity of the questionnaire was assessed using the opinion of 15 health education and promotion specialists. The content validity ratio (CVR) and content validity index (CVI) for each question was extracted and the questions were reviewed and corrected by considering the values of the Lawshe table21. Also, for the reliability of the questionnaire, in a preliminary study, the questionnaire was given to 30 students who had characteristics similar to the main study samples. Cronbach’s alpha coefficient was then calculated.
Sociodemographic variables
Sociodemographic variables included age, education, parental education, parental employment, and living status.
Waterpipe smoking
In this section, questions related to SS were presented, including the experience of SS (yes or no), history of SS in the last month (yes or no), age and place of the first SS experience. The questions of the PWM structures were analyzed using a comprehensive review of studies13,16,22-24. PWM scales on tobacco smoking were a modified version of the scales of Hukkelberg13, Gerrard16 and Bashirian25.
Positive attitude toward shisha smoking
Questions related to individual attitudes toward SS included 11 items (for example: ‘If I smoke shisha, I can concentrate more’) scored on a 5-point Likert scale with answers ranging from ‘strongly disagree’ to ‘strongly agree’. The scores of this structure ranged from 11 to 55. The highest score in this section indicated the positive attitude of students to SS. Cronbach’s alpha coefficient for the PWM structure was 0.76.
Subjective norms about shisha smoking
The questions related to subjective norms included 6 items with a score ranging from 6 to 30. Of the 6 questions, three were about the views of friends on SS, which were rated on a 5-point scale (‘I should not use at all’ to ‘I must consume’). The other three questions focused on the views of friends about SS and their influence, which were rated on a 5-point Likert scale from ‘always’ to ‘never’. The result of scores showed a positive view of friends about SS consumption and their influence. Cronbach’s alpha was estimated to be 0.86 for subjective norms.
Prototype images about shisha smokers
The questionnaire presented the prototype of an SS smoker comprising five questions describing the person in terms of intelligence, inexperienced, self-confidence, independence, and selfishness. The answers were rated on a 5-point Likert scale from ‘very much’ to ‘never’. A higher score indicated the subject’s positive prototype towards shisha smokers. Cronbach’s alpha was estimated at 81.8%.
Behavioral willingness
The questionnaire of willingness to SS includes a scenario in which an adolescent thinks that she is among her friends who are engaged in SS and they persuade her to SS. In this section, the adolescent’s reaction to this scenario was analyzed following four reactions: 1) I take the shisha pipe and smoke one or more puffs; 2) I smoke shisha with my friends until the end; 3) I thank them and I refuse to smoke; and 4) I leave that place. The answers were measured on a 5-point Likert scale ranging from ‘never’ to ‘very much’. The scores ranged from 4 to 20, respectively. A higher score indicated a greater willingness for SS by a friend’s suggestion. Cronbach’s alpha was estimated at 86.8%.
Intention to shisha smoking
There are 4 questions related to behavioral intention, which show the intention to SS the next month, the next year, trying not to use it for a lifetime, or deciding not to go to places where shisha is available (for example: ‘I may smoke a few puffs of shisha in the next month’). The scores ranged from 4 to 20, with a higher score indicating a person’s serious intention to SS. Cronbach’s alpha was estimated at 0.86 for the intention.
RESULTS
The results were obtained after completion of 1302 items by adolescent females. Respondents’ age ranged from 12 to 18 years, with a mean of 15.2 years (SD=1.9). A total of 883 (67.8%) participants reported that they had never smoked shisha, 419 (32.2%) had a single experience of SS during their lifetime, and 265 (20.4%) were current consumers of shisha. The average initiation age of SS in adolescent females in this study was 13.65 years (SD=1.7). In all, 45.8% of shisha users reported that their friend’s home was the first place they used shisha. Further sociodemographic characteristics of the participants are given in Table 1.
Table 1
Sociodemographic characteristics of participants
Mean scores, standard deviations, and correlations among the variables are presented in Table 2. There was a positive correlation between attitude and subjective norms (r=0.625; p<0.1). Also, there was a positive correlation between attitude (r=0.732; p<0.1) and subjective norms (r=0.655; p<0.1) with behavioral willingness. The results showed that behavioral willingness (r=0.817; p<0.1) and prototype (r=0.488; p<0.1) were positively correlated and significant with the intention to smoke. In addition, there were positive correlations between subjective norms (r=0.625; p<0.1) and attitude (r=0.712; p<0.1) with intention to smoke (Figure 1).
Table 2
Descriptive statistics and intercorrelations between the Prototype-Willingness Model variables (N=1302)
| Variables | 1 | 2 | 3 | 4 | 5 | Mean (SE) |
|---|---|---|---|---|---|---|
| 1 Attitude | 1 | 24.02 (9.98) | ||||
| 2 Subjective norms | 0.625** | 1 | . | 10.64 (4.93) | ||
| 3 Behavioral willingness | 0.732** | 0.655** | 1 | 9.51 (5.40) | ||
| 4 Prototypes | 0.502** | 0.417** | 0.541** | 1 | . | 12.60 (4.51) |
| 5 Behavioral intention | 0.712** | 0.625** | 0.817** | 0.488** | 1 | 8.97 (5.01) |
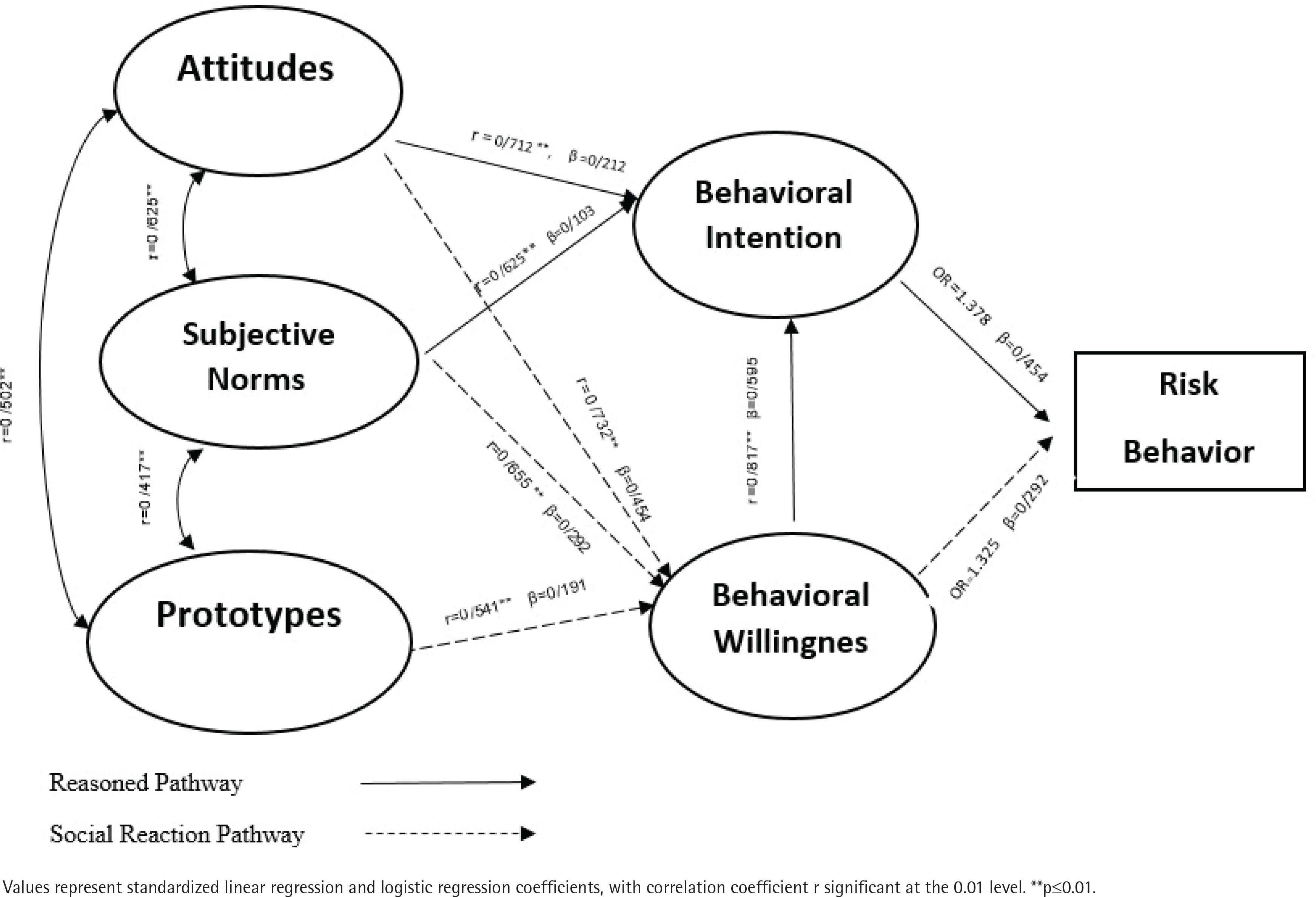
Linear regression analysis was performed to explain the variation in shisha smoking intention based in PWM (Table 3). Attitude (β=0.212; p<0.001), subjective norms (β=0.103; p<0.001) and behavioral willingness (β=0.595; p<0.001) accounted for 70% of the variance in intentions among adolescent females (Figure 1).
Table 3
Linear regression analyses predicting behavioral intention to shisha smoking (N=1302)
| Variables | β | B | SE | p | R2 |
|---|---|---|---|---|---|
| 1 Attitude | 0.212 | 0.107 | 0.012 | 0.001 | |
| 2 Subjective norms | 0.103 | 0.104 | 0.021 | 0.001 | 0.70 |
| 3 Behavioral willingness | 0.595 | 0.552 | 0.022 | 0.001 |
Table 4 shows that the PWM components accounted for 62% of the variance in willingness to shisha smoking based on the social reaction path (Figure 1). Subjective norms, attitude and prototype were the significant predictors of willingness to shisha smoking (β=0.292, p<0.00; β=0.454, p<0.001; and β=0.191, p<0.001; respectively) among adolescent females. Multiple logistic regression was employed to predict whether participants engaged with shisha smoking from: a) behavioral intention (reasoned path), or b) behavioral willingness (social reaction path). Behavioral willingness and behavioral intention significantly predicted whether participants became involved in shisha smoking (Figure 1), accounting for 74% of the variance (based on Nagelkerke R2). The behavioral intention was a better predictor of behavior (OR=1.37; p<0.001) compared to behavioral willingness (OR=1.32; p<0.001) (Table 5).
Table 4
Multiple regression analyses predicting behavioral willingness to tobacco smoking (N=1302)
| Variables | β | B | SE | p | R2 |
|---|---|---|---|---|---|
| 1 Attitude | 0.454 | 0.246 | 0.012 | 0.000 | |
| 2 Subjective norms | 0.292 | 0.319 | 0.024 | 0.000 | 0.626 |
| 3 Prototype | 0.191 | 0.229 | 0.024 | 0.000 |
DISCUSSION
This study aimed to determine the predictors of SS using PWM in adolescent females. The prevalence of SS was 32.2% in the participants who reported the experience of SS during their lifetime, which is consistent with the results of some studies22,26,27. However, the prevalence of SS experience in the present study is higher than three other studies28-30, which may be due to differences in sample size, easy access to shisha, and demographic and geographical differences in the target population.
In the present study, the prevalence of SS in current smokers in the past month was 20.4%, which was consistent with the results of other studies5,26. In past research25,31, the prevalence of SS in the past month in adolescents was 17.1%.
The mean age of SS initiation in this study was estimated to be 13.65 years, similar to the findings of three previous studies25,28,32. The average age of SS initiation in these studies was 13.8, 13.39, and 13.7 years, respectively. The results of this study showed that the initiation and tendency to use shisha begins in adolescence. Therefore, it is necessary to plan and implement effective interventions to prevent the tendency to smoke at this age.
Based on the results of this study, there is a positive and significant correlation between attitude and subjective norms with the behavioral intention, which is similar to past results33-35. This means that with positive feelings and attitudes toward SS in adolescents and the encouragement of their friends and family to SS, the intention to SS will be higher. Also, based on the findings of this study, the structures of attitude, subjective norms and behavioral willingness are effective predictors of the behavioral intention, as found by earlier research30,36. There was a study, however, where attitude could not predict the intention of behavior28, and yet, based on the reason path, attitude is expected to predict behavioral intention37. This may have originated from the study’s participants’ answers to the questions of attitude; the participants may not have expressed their true attitude towards smoking.
In this study, the analysis of the social reaction path in PWM showed that attitudes, subjective norms and positive prototype of participants predict the willingness to SS. Besides, there is a positive and significant relationship between these structures and behavioral willingness, which is consistent with the findings of earlier studies28,30,36.
The study conducted by Gerrard et al.38 on adolescent alcohol consumption shows that the prototype affects the behavioral willingness through the social reaction path and predicts behavioral willingness.
Moreover, studies25,36,39 show that when adolescents have a positive attitude towards SS and are compelled by friends and relatives to SS, friends are considered as a facilitator to create a desire to use shisha. Thus, under the pressure of others, there may be stronger willingness to engage in risky behavior without prior intention. Therefore, adolescents should learn communication skills such as ‘refusal’ and ‘saying no’ and should not respond emotionally to the issue of smoking and its suggestion by friends.
The results of this study showed that both the ‘reason path’ and the ‘social reaction path’ could predict smoking behavior. Besides, most studies of high-risk behaviors in adolescents show that both behavioral willingness and intention are strongly associated with high-risk behaviors40,41. However, according to our findings, behavioral intention can better predict SS than behavioral willingness.
Various pathways have been identified as predictors of behavior. In some studies30,40,42, the behavioral intention has been introduced as an important predictor of behavior, which is consistent with the present study. However, other studies28,32 reported behavioral willingness as a more important predictor of behavior.
Another study14 suggests that at a young age (13 years), when adolescents have little experience with smoking, the willingness can predict behavior more efficiently than intention. With increasing experience and higher age (16 years), the role of the behavioral intention becomes more prominent. At the same time, although behavioral enthusiasm has not diminished, its role in predicting behavior is less important than behavioral intention.
Limitations
Limitations of the study include that data collection was based on a self-reporting questionnaire, which may raise the possibility of recall and response bias. We tried to resolve this issue by emphasizing the confidentiality and anonymity of the information obtained through the questionnaires.
CONCLUSIONS
Considering the increasing popularity of SS among adolescent females and its increasing prevalence, it is required to design and implement programs to prevent SS. Also, it is necessary to consider the influence of PWM structures, such as behavioral intention and willingness, on the tobacco issue when designing educational strategies.