INTRODUCTION
Smoking is one of the leading preventable causes of death worldwide1. More than 0.7 million Europeans die prematurely as a result of smoking-related illnesses each year2. The European Commissions’ latest Special Eurobarometer reported that 46.0% of tobacco users in Europe have never tried to quit smoking and only 15.0% of current tobacco users reported having made a quit attempt during the past year3. Among those who have attempted to quit smoking, the majority (75%) reported they did so unassisted3. Only a small percentage of those who quit unassisted will maintain long-term abstinence from smoking4-6. As a chronic relapsing condition, tobacco dependence treatment is difficult and multi-factorial7,8.
Health care professionals have an important role to play in the delivery of tobacco treatment interventions2,4,9. There is strong evidence that the combination of clinician’s advice to quit smoking, pharmacotherapy and behavioral counseling can increase success with long-term abstinence three- to six-fold4,9-11. In this context, both the World Health Organization and the European Network for Smoking and Tobacco Prevention (ENSP) have identified tobacco dependence treatment as a clinical priority for all healthcare professionals and recommend that all health care providers be trained in evidence-based tobacco treatment delivery and be prepared to intervene with tobacco users in their practice2,9,12,13. Despite the importance of this area of clinical practice, the vast majority of clinicians in Europe have not received training in tobacco treatment delivery14. Continuing medical education has proven to be effective in changing health care professionals’ behaviors in integrating tobacco treatment delivery into daily clinical practice and increasing patient success with quitting15-17.
Similar interventions in terms of the content and the tools used have been performed in the past. The ‘Ottawa Model for Smoking Cessation’ (OMSC), is a multi-component intervention for addressing tobacco use with smokers in primary care settings in Canada. Its evaluation has demonstrated significant improvements in the rates at which evidence-based tobacco treatment is delivered to patients17,18 , while TiTAN Crete is a European study that adapted the OMSC program for use in primary care settings and developed a network of trained general practitioners (GPs) in Crete, Greece, to integrate treatment of tobacco dependence into daily clinical practice. The results of TiTAN Crete demonstrated that the training intervention was effective in improving a GP’s knowledge, self-efficacy and delivery of the 4As (ask, advise, assist, arrange) tobacco treatment19.
The aim of this study was to assess the short-term effectiveness of the EuroPean Accredited Curriculum on Tobacco Treatment Training intervention in improving health care provider’s knowledge, attitudes and self-efficacy related to tobacco dependence treatment.
METHODS
A pre–post pilot study was conducted. This study was undertaken as part the EuroPean Accredited Curriculum on Tobacco Treatment (EPACTT) project. The purpose of EPACTT was to create and mobilize a network of healthcare professionals, dedicated to advancing evidence-based tobacco dependence treatment and advocating for effective tobacco control policy in the Eastern European Region with specific focus on clinician and policy makers in Russia, Ukraine, Georgia, Armenia and Romania.
The training intervention was held in Brussels, Belgium in April 2016. Participants were asked to complete an online study questionnaire at three time points, before the intervention (Τ1–March 2016), immediately after (Τ2–April 2016) and two months following the training (Τ3–June 2016).
Recruitment
A convenience sample of health care professionals was recruited from the six participating European countries (Russia, Ukraine, Georgia, Armenia, Romania and Greece). The lead representatives from each country were asked to identify a list of ten health care professionals to participate in the pilot study. Eligibility criteria included: 1) being a health care professional (i.e. general practitioners, nurses, midwives, psychologists, social workers, pharmacists); 2) ability to read and comprehend English; 3) currently working with smokers on a daily basis; and 4) able to participate in the training event in Brussels. Each of the identified health care professionals received an information letter and an invitation to participate via email with a link to the baseline survey. All healthcare professionals were required to provide informed consent and completed the baseline survey. Participants also completed a printed survey at the end of the second day of the training. Two months following the training, participants were contacted via email with a link to the follow-up survey. Three email reminders were sent over a three-week period before categorizing the participant as loss to follow-up.
Intervention and evaluation framework
The training intervention and evaluation design was informed by behavioral theory and existing research, in terms of the process by which training interventions are thought to influence provider behaviors20,21. Specifically, we sought to influence provider’s knowledge, attitudes and confidence (selfefficacy) related to the delivery of evidence-based tobacco treatment22,23. We also evaluated social norms in terms of the importance of tobacco control within clinical practice. Each of the areas targeted have been identified in the literature as barriers to tobacco treatment delivery22,25,26.
Training intervention
The intervention was based on the 2015 European Tobacco Treatment Guidelines published by the European Network for Smoking and Tobacco Prevention (ENSP) and was designed to meet multidisciplinary needs and to provide knowledge and skills to support the integration of evidence-based tobacco treatment into daily clinical practice13. The two-day training program was delivered by tobacco treatment experts who were involved in the development of the ENSP clinical practice guidelines. The training program covered the following learning areas: 1) data on the tobacco epidemic in Europe, 2) health effects of tobacco use, 3) pathophysiology of addiction to nicotine, 4) the role of health care professionals in tobacco control, 5) evidence-based practices for tobacco treatment delivery including counseling techniques and pharmacotherapy, 6) tobacco control legislation and enforcement on an international and European level, and 7) standards for the establishment and operation of a smoking cessation clinic. Active learning methods such as teaching role-play and case studies were used as part of the training intervention.
Evaluation tool
The baseline study survey collected information about the demographics of health professionals, such as gender, age, smoking status, number of years practicing as well as previous training in smoking cessation. At time points T1, T2 and T3 we assessed provider knowledge (12 items), attitudes (10 items), perceived behavioral control (5 items), and self-efficacy (6 items) related to tobacco treatment delivery. All knowledge questions were based on the 2015 European Network on Smoking Cessation Guidelines13. The survey instrument was originally a modification of an existing tool developed by Papadakis et al.22,23, and builds on the work of Delucchi and others24,27. The survey instrument was adapted for use in European health care settings.
Statistical analysis
Frequencies and percentages were used to summarize demographic characteristics of the sample and outcomes variables at time points T1, T2 and T3. Data reported on a 5-point Likert scale (1=strongly disagree, 2=disagree, 3=neutral, 4=agree, 5=strongly agree) were recoded as follows: strongly disagree and disagree=disagree; neutral=neutral; strongly agree and agree=agree. Chi-squared tests were performed to evaluate the effectiveness of the intervention in improving health care professionals’ knowledge, attitudes, perceived behavioral control, self-efficacy (a 10-point Likert scale was used with 1=not very confident to 10=extremely confident) before and immediately after the intervention (T1 vs T2) and at 2 months following the intervention (T1 vs T3). For the analysis of continuous data, we performed Kolmogorov-Smirnov test to check for the normality of our data and analysis of variance (ANOVA) was performed. Statistical significance was set at 0.05. Only those health care professionals (n=40) who completed the training and follow-up surveys were included in the final analysis. Missing data were not imputed. Statistical analysis was performed using the Statistical Package for Social Sciences (SPSS, 21st Edition).
RESULTS
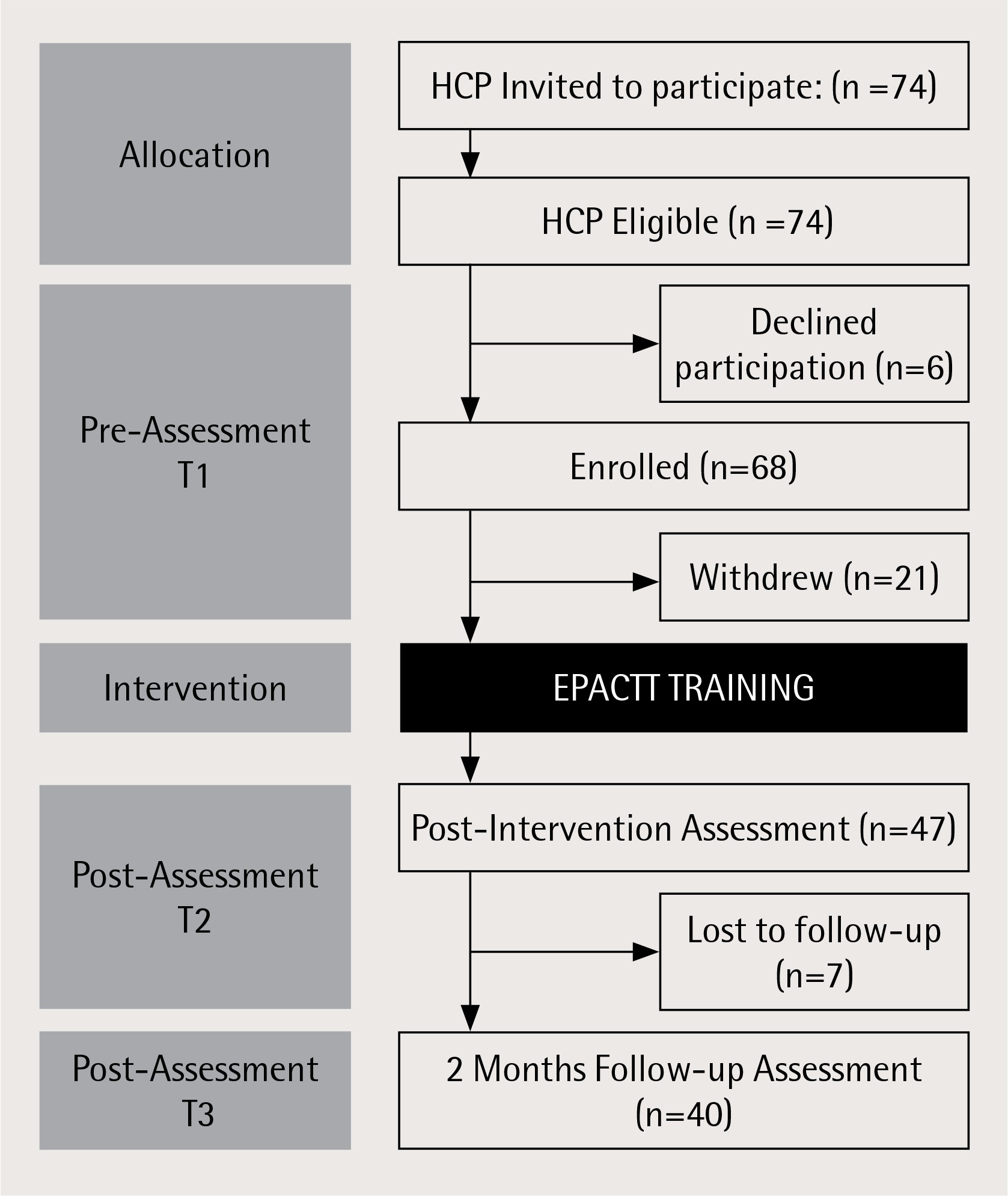
The recruitment flow diagram is presented as Figure 1. A total of 68 health care professionals consented to participate in the study, of which 47 attended the training intervention while 7 were lost to follow-up (69.1% retention rate). The primary reason for withdrawal from the study was inability to travel to the training event. It should be noted that the week prior to the training event a terrorist attack occurred in Paris, which resulted in many participants canceling their travel.
Supplementary Table 1 depicts the demographic and descriptive characteristics of the study participants. The majority (77.5%) of participants were women and 40% of the sample worked in a hospital. Participants had been practicing for an average of 21.4 (SD=24.2) years. The majority of the sample (62.5%) had not previously participated in training on smoking cessation.
Table 1
Changes in health care professionals’ tobacco treatment knowledge after the training intervention, Brussels, Belgium (n=40)
Increases were documented in 11 of the 12 knowledge areas assessed immediately following the training, with significant increases documented in 3 of the 12 areas assessed: pharmacotherapy effectiveness (5.1% at T1 vs 70% at T2, p<0.001); craving duration (41.0% at T1 vs 72.5% at T2, p=0.005); relapse reason (66.7% at T1 vs 87.5% T2, p=0.027) (Table 1). For three of the knowledge areas less than 50% of participants responded correctly. Comparisons between the assessment before training (T1) and at the 2 months follow-up (T3) indicate that knowledge was not retained by all participants: pharmacotherapy effectiveness (5.1% at T1 vs 59% at T3, p<0.001); craving duration (41.0% at T1 vs 59% at T3, p=0.113); relapse reason (66.7% at T1 vs 69.2% at T3, p=0.808)
Positive changes in most items assessing provider attitudes related to tobacco treatment delivery significantly increased between the pre-assessment (T1) and immediately after the intervention (T2), however significant increases were observed in only 2 of the 10 items assessed: smoking cessation follow up (T1 vs T2, p=0.032; T1 vs T3, p=0.022); pharmacotherapy effectiveness (T1 vs T2, p<0.001; T1 vs T3, p=0.023) (Table 2).
Table 2
Changes in tobacco related attitudes and perceived behavioral control among participants before, immediately after, and at 2 months following exposure to the training intervention, Brussels, Belgium (n=40)
| T1 | T2 | T1 vs T2 | T3 | T1 vs T3 | |
|---|---|---|---|---|---|
| Variable | Pre % (n) | Post % (n) | p | At 2 months follow-up % (n) | p |
| Attitudes Helping my patients quit smoking is an important part of my role as a clinician | |||||
| Disagree | 0.0 (0) | 0.0 (0) | 0.221 | 2.7 (1) | |
| Neutral | 17.9 (7) | 8.3 (3) | 10.8 (4) | 0.413 | |
| Agree * | 82.1 (32) | 91.7 (33) | 86.5 (32) | ||
| Clinicians should advise patients to quit smoking even if it’s not the reason for the visit | |||||
| Disagree | 2.8 (1) | 2.6 (1) | 0. 206 | 2.6 (1) | |
| Neutral | 13.9 (5) | 2.6 (1) | 2.6 (1) | 0.206 | |
| Agree * | 83.3 (30) | 94.7 (36) | 94.7 (36) | ||
| Counseling by a clinician helps motivate smokers to quit | |||||
| Disagree | 8.3 (3) | 0.0 (0) | 0.0 (0) | ||
| Neutral | 13.9 (5) | 5.3 (2) | 0.073 | 5.4 (2) | 0.080 |
| Agree * | 77.8 (28) | 94.7 (36) | 94.6 (35) | ||
| Clinicians should make appointments specifically to help patients quit | |||||
| Disagree | 0.0 (0) | 2.6 (1) | 5.3 (2) | ||
| Neutral | 30.6 (11) | 7.9 (3) | 0.032 | 7.9 (3) | 0.022 |
| Agree * | 69.4 (22) | 89.5 (34) | 86.8 (33) | ||
| Smoking is a personal decision that does not concern the clinician | |||||
| Disagree * | 60.5 (23) | 60.5 (23) | 0.934 | 84.2 (32) | |
| Neutral | 18.4 (7) | 15.8 (6) | 7.9 (3) | 0.069 | |
| Agree | 21.1 (8) | 23.7 (9) | 7.9 (3) | ||
| For many tobacco users smoking is an addiction | |||||
| Disagree | 3.0 (1) | 10.5 (4) | 5.6 (2) | ||
| Neutral | 24.2 (8) | 10.5 (4) | 0.177 | 8.3 (3) | 0.185 |
| Agree * | 72.7 (24) | 78.9 (30) | 86.1 (31) | ||
| A patient’s will power alone is what will determine their success with quitting | |||||
| Disagree * | 31.0 (9) | 50.0 (19) | 0.102 | 50.0 (19) | 0.294 |
| Neutral | 41.4 (12) | 18.4 (7) | 28.9 (11) | ||
| Agree | 27.6 (8) | 31.6 (12) | 21.1 (8) | ||
| First line pharmacotherapies for smoking cessation work well in helping patients quit | |||||
| Disagree | 0.0 (0) | 7.9 (3) | <0.001 | 2.6 (1) | |
| Neutral | 48.4 (15) | 5.3 (2) | 18.4 (7) | 0.023 | |
| Agree * | 51.6 (16) | 86.8 (33) | 78.9 (30) | ||
| First line pharmacotherapies for smoking cessation are not safe, have side effects that out weight their benefits | |||||
| Disagree * | 55.6 (20) | 60.5 (23) | 0.121 | 13.2 (5) | 0.103 |
| Neutral | 36.1 (13) | 18.4 (7) | 18.4 (7) | ||
| Agree | 8.3 (3) | 21.1 (8) | 68.4 (26) | ||
| It is my usual practice to assist my patients to quit smoking | |||||
| Disagree | 0.0 (0) | 8.3 (3) | 5.3 (2) | 0.327 | |
| Neutral | 21.9 (7) | 16.7 (6) | 0.231 | 18.4 (7) | |
| Agree * | 78.1 (25) | 75.0 (27) | 55.3 (21) | ||
| Perceived behavioral control | |||||
| I have the required skills to help my patients quit smoking | |||||
| Disagree | 0.0 (0) | 0.0 (0) | 0.003 | 2.6 (1) | |
| Neutral | 38.7 (12) | 8.3 (3) | 13.2 (5) | 0.038 | |
| Agree* | 61.3 (19) | 91.7 (17) | 84.2 (32) | ||
| My patients follow my advice about behavior change smoking | |||||
| Disagree | 0.0 (0) | 0.0 (0) | 0.005 | 5.3 (2) | |
| Neutral | 48.5 (16) | 16.7 (6) | 26.3 (10) | 0.085 | |
| Agree* | 51.5 (17) | 83.3 (30) | 68.4 (26) | ||
| My patients who smoke want to quit smoking | |||||
| Disagree | 2.8 (1) | 5.6 (2) | 7.9 (3) | ||
| Neutral | 66.7 (24) | 36.1 (13) | 0.035 | 28.9 (11) | 0.005 |
| Agree* | 30.6 (11) | 58.3 (21) | 63.2 (24) | ||
| I do not feel I have an effective method to assist my patients with quitting | |||||
| Disagree* | 28.6 (10) | 67.6 (25) | <0.001 | 57.9 (22) | 0.028 |
| Neutral | 54.3 (19) | 13.5 (5) | 26.3 (10) | ||
| Agree | 17.1 (6) | 18.9 (7) | 15.8 (6) | ||
| I know where to refer patients for help with smoking cessation | |||||
| Disagree | 15.4 (6) | 16.2 (6) | 0.003 | 13.2 (5) | 0.010 |
| Neutral | 48.7 (19) | 13.5 (5) | 18.4 (7) | ||
| Agree* | 35.9 (14) | 70.3 (26) | 68.4 (26) |
Significant increases were documented in all of the perceived behavioral control items assessed at the end of training: smoking cessation skills (T1 vs T2, p=0.003; T1 vs T3, p=0.038); patient compliance (T1 vs T2, p=0.005; T1 vs T3, p=0.085); desire to quit smoking (T1 vs T2, p=0.035; T1 vs T3, p=0.005); smoking cessation methods (T1 vs T2, p<0.001; T1 vs T3, p=0.028); patient referral (T1 vs T2, p=0.003; T1 vs T3, p=0.010) (Table 2). Immediately after the intervention, health care professionals were significantly more confident in their ability to deliver evidence-based tobacco treatment with significant increases observed in all self-efficacy items assessed following training, with the exception of arranging timely follow-up support for patients (Table 3). These changes remained significant at the two months follow-up.
Table 3
Changes in health care professionals’ self-efficacy related to tobacco treatment delivery following exposure to the training intervention, Brussels, Belgium (n=40)
DISCUSSION
The results of our study showed that an evidence-based training program is effective in significantly increasing health care professionals’ confidence in their ability to deliver evidence-based tobacco treatment to their patients who smoke. Following the training, more than 90% of participants reported that they felt that they had the required skills to help their patients to quit smoking, a significant increase documented relative to baseline (61.3% vs 91.7%; p=0.001).
While there was a significant improvement in self-efficacy in all areas of evidence-based tobacco treatment delivery, the average score for motivating patients not ready to quit smoking and prescribing quit- smoking medications suggests that there is room for further improvement. Importantly, we did not document a significant increase in provider confidence to arrange timely follow-up for patients embarking on a quit attempt. This suggests factors outside the training may influence provider’s confidence in their ability to delivery follow-up support to patients. This important finding should be further explored.
While there was an overall increase in provider knowledge documented across the 12 domains assessed, in 4 of the knowledge questions less than 50% of providers responded correctly at follow-up (T3). While each individual knowledge area may not be critical to tobacco treatment delivery, future training and evaluation work should ensure that critical areas of knowledge are emphasized within the training program to a greater extent.
Positive increases were documented in several of the provider ‘attitudes’ thought to be associated with the frequency at which health care professionals deliver tobacco treatment following exposure to the training. We did not, however, document significant improvements in all of the provider ‘attitudes’ assessed. Future research should examine intervention strategies for influencing health care provider attitudes and intentions related to tobacco treatment delivery, which may include tactics in addition to training.
Several studies have indicated that negative attitudes and a lack in both knowledge and confidence in tobacco treatment are common among health care professionals and are barriers to tobacco treatment delivery5,25,28-32. In the present study the majority of health care professionals had not previously received training in tobacco treatment, reported low baseline knowledge in several areas assessed, had poor attitudes, and low self-efficacy related to smoking cessation counseling and in prescribing quit-smoking medications. These data support the importance of interventions such as that assessed as part of the EPACTT program.
The results of our study are in agreement with other studies, which reported improved knowledge and skills in counseling for smoking cessation following training33-36. A large survey conducted in 2014 at 146 smoking cessation centers showed that both online and face-to-face interventions can effectively improve the knowledge and skills of health care professionals37. There is good evidence that health care professionals who receive training on smoking cessation are more likely to deliver smoking cessation counseling, and are more likely to use evidence-based tobacco treatment techniques17,36. There was a decline in some of the knowledge domains observed between the post-training and at the 2 months follow-up assessment, which may support the need for additional training over time to maintain tobacco treatment knowledge.
This study is subject to certain methodological limitations. It is unclear whether health care professionals participated in our intervention are representative of the general population, as most of them were members of European organizations for smoking prevention. Our pilot study included a relatively small sample size that may also limit the generalization of the results. The survey instrument was based on existing knowledge of provider behavior change in terms of tobacco treatment delivery, however this is an under-studied area of research and there may be other factors not measured in our study that influence provider behaviors. Given the survey was anonymous and completely voluntary, one can assume that attitudinal variables were reliably captured38.
CONCLUSIONS
The results of this pilot study demonstrate that tobacco treatment training is able to improve health professional’s knowledge and self-efficacy related to smoking cessation treatment. Ongoing training and other intervention tactics may be necessary to maintain and further improve provider knowledge, attitudes and skills.